

The CSiM Exchange
Advancing Stewardship, Quality, and Collaboration in Rural Health.
Our quarterly newsletter brings together timely updates in stewardship, infectious diseases, and rural health, highlighting practical tools and emerging topics designed to support clinicians and partners serving rural communities.
In this Spring 2026 issue you can find:
- Measles Activity in the United States: A Continuing Public Health Emergency
- By the Numbers: Leveraging the Urinalysis to Understand True Antibiotic Overuse
- Nursing Education and Stewardship Implementation
- Save the Date! CSiM conference Friday, September 25, 2026 in Spokane, WA
The CSiM Exchange is open to current partners, past participants, and those newly engaging with our work. If you are interested in learning more, email us at uwcsim@uw.edu
We look forward to continuing to share resources and insights to strengthen stewardship, quality improvement, and rural health systems.
Measles Activity in the United States: A Continuing Public Health Emergency

by John B Lynch, MD, MPH
The United States is experiencing its most severe measles resurgence in more than three decades. From January 1, 2025, through late March 2026, over 3,860 confirmed measles cases were reported across 46 states and jurisdictions, with approximately 93% occurring in people who were unvaccinated or whose vaccination status was unknown.
In 2025, 2,285 confirmed cases were reported, the most since 1991. As of early April 2026, an additional 1,671 confirmed cases have been recorded for this year alone, with 94% linked to ongoing outbreaks. Critically, whereas 40% of measles cases were imported during the elimination period of 2001–2011, only about 10% were imported in 2025 and just 6% in 2026, signaling that local, sustained community transmission has become the dominant driver of spread.
Four deaths have now been confirmed: two unvaccinated children in Texas, one unvaccinated adult in New Mexico, and one child in Los Angeles County who died from a measles-related complication. The demographic profile skews heavily toward children: 21% of 2026 cases are in children younger than five, and 74% involve children and young adults up to age 19, with 92% of all case-patients either unvaccinated or of unknown vaccine status. Underlying the outbreak is a steady erosion of population immunity: MMR vaccination coverage among U.S. kindergartners has declined from 95.2% during the 2019–2020 school year to 92.5% in 2024–2025, leaving an estimated 286,000 kindergartners unprotected.
Sustaining measles elimination requires community-level coverage above 95%; CDC data from 2025 found coverage in some affected Texas counties had fallen below 82%. A recent county-level analysis published in Nature Health using participatory surveillance data found even more concerning gaps: county-level MMR uptake estimates ranged from 35.8% to 86.8%, with the lowest coverage concentrated in West Texas, southern New Mexico, northern Arizona, parts of Mississippi, and the rural Southeast, the same regions experiencing the most significant outbreaks. The United States is now formally at risk of losing its measles elimination status, which it has held since 2000.
Rural Vulnerabilities
Rural communities face a compounding set of risk factors that make measles containment especially challenging. The initial 2025 cluster was identified in Gaines County, Texas, a largely rural area home to a substantial Mennonite farming community where vaccination rates have historically trailed the national average, and rural access barriers, including limited pediatric provider availability, affected immunization completion rates.
In 2025, some rural counties with healthcare provider shortages experienced delayed diagnoses, which allowed wider spread, and rural hospitals that furloughed exposed non-immune healthcare workers per CDC guidance were often unable to backfill shifts, forcing diversion of febrile-rash patients. Researchers have noted that national vaccination rate estimates may not capture homeschooled or some undocumented children, who are less likely to be vaccinated, meaning true community immunity may be lower than currently reported.
Measles the Pacific Northwest
Washington and Oregon are reporting active measles transmission in 2026. Washington has recorded 26 measles cases since the start of 2026, more than double the state’s total for all of 2025, with cases identified in four counties and the majority concentrated in Snohomish County, predominantly among unvaccinated children. Washington’s kindergarten MMR vaccination rate for 2024–2025 stands at approximately 91%, well below the 95% threshold required for herd immunity. Oregon has confirmed 13 cases as of early April 2026, with recent exposures occurring across the Portland metro area, though state and university experts believe confirmed cases represent only a fraction of true incidence, as not everyone who contracts measles seeks medical care and receives a diagnosis.
The Oregon Health Authority has noted sporadic detections of measles virus in wastewater surveillance since October 2025, reinforcing concern that community circulation is broader than case counts suggest. Vaccination rates in Oregon vary widely: approximately one in 15 kindergartners has received no dose of the MMR vaccine, and one in 10 has received only one dose, with rates significantly lower in specific communities and schools.
Clinicians should maintain a high index of suspicion for measles in any patient presenting with fever and rash, particularly in unvaccinated individuals, and should contact patients by phone before an in-office visit to prevent inadvertent exposure in healthcare settings. Post-exposure MMR vaccination within 72 hours and immunoglobulin within six days remain the cornerstones of outbreak response for susceptible contacts.
- https://publichealthcollaborative.org/communication-tools/communicating-about-the-2025-measles-outbreak/
- https://www.cdc.gov/measles/data-research/index.html
- https://www.kff.org/other-health/measles-elimination-status-what-it-is-and-how-the-u-s-could-lose-it/
- https://stacks.cdc.gov/view/cdc/255122
- https://www.nejm.org/doi/full/10.1056/NEJMra2504516
- Video: https://www.facebook.com/TheNewEnglandJournalofMedicine/videos/measles/856931127044457/
- https://www.cdc.gov/infection-control/hcp/healthcare-personnel-epidemiology-control/measles.html
- https://www.cdc.gov/infection-control/hcp/measles/index.html 4).
By the Numbers: Leveraging the Urinalysis to Understand True Antibiotic Overuse
Whitney Hartlage, PharmD, reframes how to identify inappropriate prescribing by introducing ASPN, a urinalysis-based approach that better aligns with real-world clinical decision-making. See how this shift can uncover missed opportunities and strengthen stewardship in practice. No CSiM subscription required
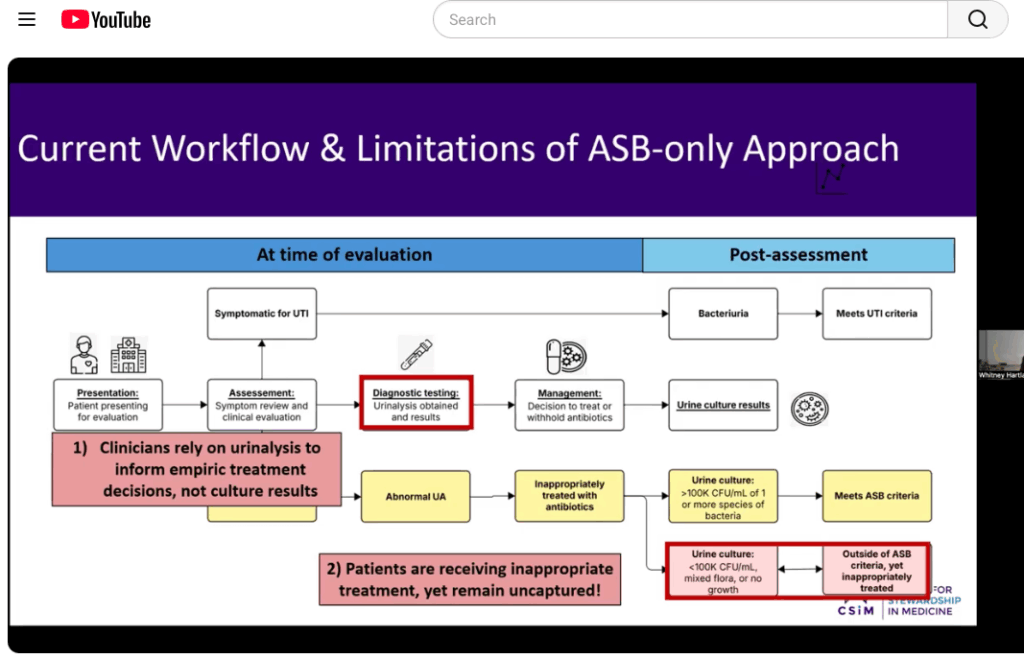
UTI Stewardship Gaps
- 7M+ emergency department visits annually for UTIs in the U.S.
- 2.88M hospitalizations each year
- 20–60% of patients may be treated without clear symptoms
- 53% of inappropriate treatment captured using ASB
- 89% captured using ASPN (urinalysis-based metric)
- 16% of inappropriately treated patients had no growth on culture
Nursing Education and Stewardship Implementation
On April 28, Dr. Zahra Kassamali Escobar hosted a nurse panel featuring Emily Williamson, RN, BSN, OHCC, and Barbara MacDonald, RN, CIC, both from participating Critical Access Hospitals, who shared how frontline clinical judgment drives better antibiotic use. From pausing before ordering a urinalysis to reassessing antibiotics at 48 hours and strengthening communication with providers, these everyday decisions play a critical role in stewardship.
Click here to access panel discussion. Must have current CSiM subscription to access
A friendly reminder that the CSiM Nursing Curriculum is available and ready for use. Please share these resources across your hospital, and let us know if we can help support implementation.
Stewardship Education for Nurses
Save the Date! September 25, 2026
CSiM Conference September 25, 2026 in Spokane, WA
We’re excited to announce the return of the UW CSiM Conference held at the Spokane DoubleTree by Hilton Spokane City Center. Registration, draft agenda, and lodging information will be shared in early summer.
This free, one-day event is open to all with an interest in rural health and antimicrobial stewardship. We welcome current and past CSiM participants, as well as anyone working to support rural healthcare communities.
There will be sponsorship opportunities for travel and lodging for current UW CSiM participants. Stay tuned for more information in early summer.